
Clitoral Adhesions: Causes, Symptoms & Pelvic Floor Physiotherapy Treatment
Clitoral adhesions are one of the most underdiagnosed and most undertalked about conditions in women's sexual health. Many women live for years with unexplained clitoral pain, reduced sensation, difficulty reaching orgasm, or discomfort during intimacy, never receiving a clear diagnosis. In many of these cases, clitoral adhesions are the missing piece of the puzzle.
At our specialized pelvic pain clinic, we see this condition regularly, and we want every woman to know: your symptoms are real, they have a name, and in most cases, they have a treatment.
This complete guide covers everything you need to know about clitoral adhesions, what they are, why they happen, what they feel like, and how pelvic floor physiotherapy can help you find lasting relief.
⭐ Key Takeaways
Clitoral adhesions occur when the clitoral hood gets stuck to the glans clitoris, restricting natural movement and reducing sensation.
They are found in approximately 22% of women seeking help for sexual dysfunction, far more common than most people realize.
Symptoms include clitoral pain (clitorodynia), reduced or absent orgasm, hypersensitivity, and pain during or after sex
Common causes include smegma and keratin pearl buildup, lichen sclerosus, lichen planus, hormonal changes, and trauma to the vulvar area.
Clitoral adhesions frequently co-occur with vulvodynia, provoked vestibulodynia, pudendal neuralgia, and pelvic floor muscle dysfunction.
Treatment options range from non-surgical lysis and topical therapies to clitoral prepuce myofascial release and specialized pelvic floor physiotherapy.
With the right care, most women experience meaningful improvement in comfort, sensation, arousal, and quality of life.
🎥 Watch: Clitoral Adhesions: Why It Happens & How Physio Treats It
Clitoral adhesions are one of the most underdiagnosed causes of clitoral pain, reduced sensation, and difficulty with orgasm in women, present in approximately 22% of those seeking help for sexual dysfunction. This video from our pelvic floor physiotherapy team in Burnaby covers the full picture: causes, symptoms, and evidence-based treatment options, including clitoral prepuce myofascial release and pelvic floor physiotherapy.
What Are Clitoral Adhesions?
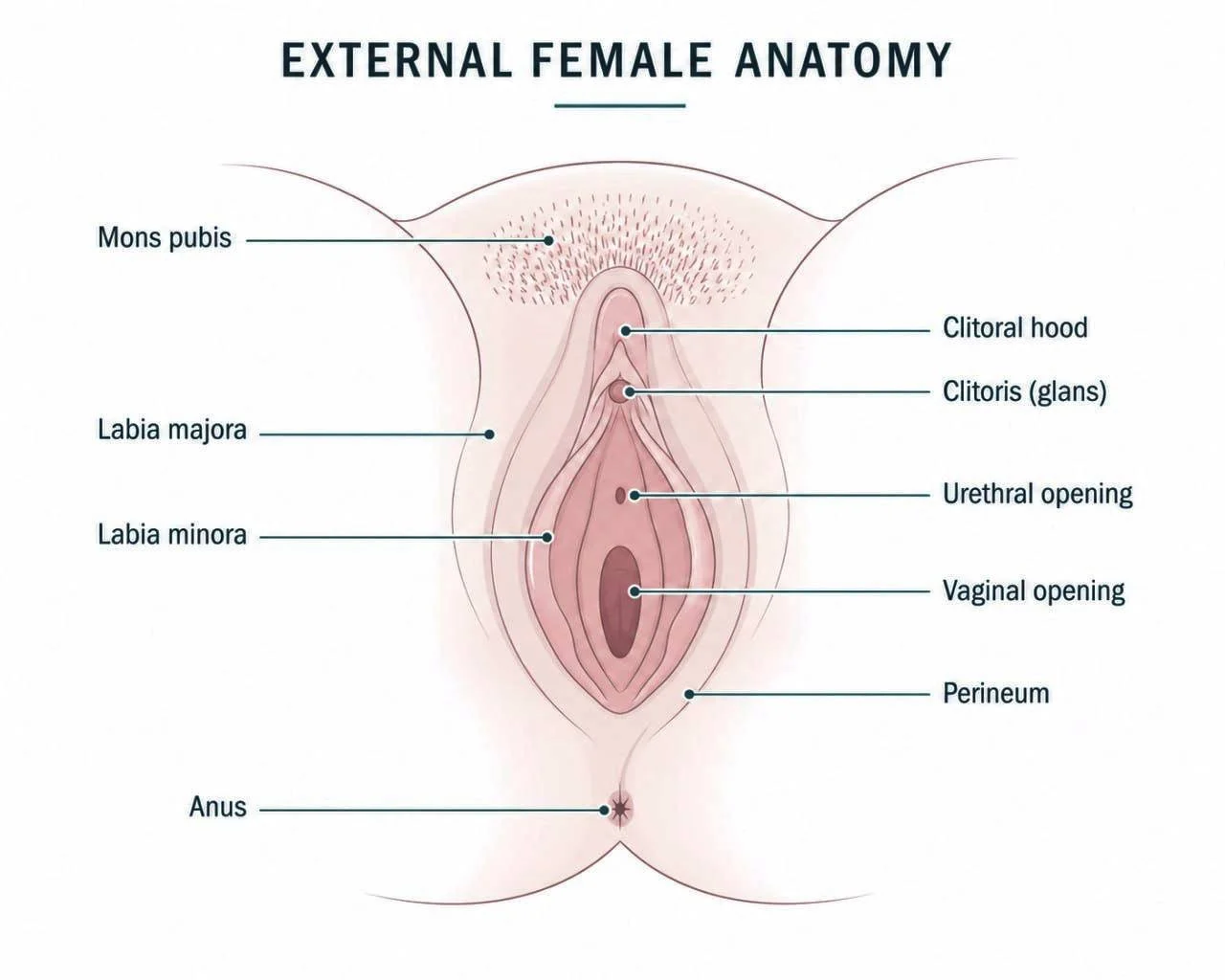
The clitoris has a highly sensitive tip called the glans clitoris, which is normally covered and protected by a retractable fold of skin known as the clitoral hood (or prepuce). Under healthy conditions, this hood moves freely, retracting during sexual activity to allow stimulation of the glans, and returning to its protective position afterward.
A clitoral adhesion occurs when the clitoral hood becomes fused to the glans clitoris, either partially or completely, preventing this natural retraction. When the hood and glans stick together, debris such as smegma (a natural mixture of dead skin cells, oils, and fluids) and hardened keratin pearls can become trapped underneath, leading to irritation, inflammation, pain, and restricted sensation.
This condition is also sometimes called clitoral phimosis when the hood can no longer retract at all. While it may sound like a minor anatomical issue, the clitoris is the primary erogenous zone of the vulva, and any restriction to its function can profoundly affect comfort, arousal, orgasm, and overall sexual well-being.
How Common Are Clitoral Adhesions?
Clitoral adhesions are far more prevalent than most people, including many healthcare providers, realize. Research published in Sexual Medicine Reviews found they are present in approximately 22% of women presenting for sexual dysfunction evaluation, and in 33% of female college students during routine pelvic examination.
Despite these numbers, clitoral exams are still not routine in most clinical settings, which means this condition is widely missed and often misattributed to anxiety, relationship issues, or vague diagnoses that never quite fit. If you have been told your symptoms are unexplained, clitoral adhesions deserve proper investigation.
What Causes Clitoral Adhesions?
Clitoral adhesions can develop for a variety of reasons, and in most cases, they result from a combination of factors rather than a single cause.
• Smegma Buildup and Keratin Pearls:
Smegma is a naturally occurring mixture of skin oils, dead cells, and moisture that collects under the clitoral hood. When it is not regularly cleared, either due to hygiene difficulty or anatomical factors, it can harden into keratin pearls: small, sand-like granules that become trapped between the hood and the glans and cause the two surfaces to fuse together over time.
• Lichen Sclerosus:
A chronic inflammatory skin condition that primarily affects the vulvar area, causing the skin to become thin, pale, and fragile. Lichen sclerosus significantly increases the risk of scarring and adhesion formation, and is more common in postmenopausal women, though it can occur at any age.
• Lichen Planus:
Another inflammatory skin condition that can affect the genitals, causing tissue changes that contribute to adhesion development over time.
• Hormonal Changes:
Declining estrogen during perimenopause, menopause, the postpartum period, or while using certain hormonal medications causes vulvar tissues to thin, dry out, and lose elasticity. This makes the tissue far more vulnerable to irritation and adhesion formation, a process sometimes called genitourinary syndrome of menopause (GSM).
• Trauma or Injury:
Physical trauma to the vulvar area, including perineal injuries during childbirth, prior vulvar surgeries, or blunt genital trauma, can cause scarring and subsequent adhesion formation.
• Chronic Irritation:
Ongoing friction from tight clothing, synthetic fabrics, or harsh soaps can cause repeated low-grade inflammation in the vulvar area that, over time, contributes to tissue changes and adhesions.
• Recurrent Infections:
A history of recurrent yeast infections or urinary tract infections has been identified as a risk factor, likely due to the chronic inflammatory environment they create.
Symptoms of Clitoral Adhesions
Symptoms can range from absent in mild cases to significantly life-affecting. Every woman's experience is different, but common presentations include:
• Clitoral Pain (Clitorodynia):
A persistent aching, burning, sharp, or stabbing sensation in the clitoral area, either at rest or triggered by touch, clothing contact, or stimulation.
• Reduced Sensation or Numbness:
A dulling of clitoral sensitivity where stimulation that once felt pleasurable no longer has the same effect. This often happens because the adhesion physically prevents the glans from being properly accessed or stimulated.
• Hypersensitivity:
Some women experience the opposite — extreme sensitivity where even light touch or clothing contact produces significant discomfort or pain.
• Difficulty Reaching Orgasm or Absent Orgasm:
Because the clitoris plays such a central role in female sexual response, adhesions that restrict its mobility can make arousal more difficult and orgasm harder to achieve or absent altogether.
• Pain During or After Sex:
Pain during or after sexual activity is a common concern, often due to tension or pulling around the restricted clitoral hood during intimacy.
• Visible Changes:
Some women notice that the clitoral hood does not retract as freely as it once did, or observe redness, swelling, or discharge from the area.
• General Vulvar Discomfort:
An ongoing sense of irritation, aching, or pressure in the vulvar area that is not clearly tied to any specific activity.
If any of these symptoms sound familiar, you are not alone, and you do not have to keep living with them.
The Connection Between Clitoral Adhesions and Pelvic Floor Dysfunction
One of the most important findings in recent research is that clitoral adhesions rarely exist in isolation. They are frequently found alongside other pelvic pain conditions, which is why a thorough pelvic floor assessment is so essential for anyone presenting with clitoral pain or sexual dysfunction.
Common co-occurring conditions include vulvodynia, provoked vestibulodynia (PVD), pudendal neuralgia and interstitial cystitis. Painful orgasm (dysorgasmia) is also associated with the same underlying muscle tension and nerve sensitization that develops over time.
Perhaps most importantly, chronic clitoral pain almost always leads to overactive pelvic floor muscle dysfunction. When the body is in persistent pain, it protects itself by tightening the surrounding muscles. Over time, this guarding becomes automatic, happening even on days when pain feels lower and creates its own cycle of increased sensitivity, restricted movement, and worsened sexual function. This is one of the key reasons pelvic floor physiotherapy plays such a central role in treatment.
How Are Clitoral Adhesions Diagnosed?
Diagnosis begins with a thorough clinical examination by a provider who is knowledgeable about vulvar conditions. A proper clitoral exam assessing whether the hood retracts normally and checking for the presence of smegma, keratin pearls, or fused tissue should be part of any comprehensive pelvic health assessment.
Because this exam is not yet standard practice in most clinical settings, many women go years without receiving it. If you have unexplained clitoral pain, changes in sensation, or sexual dysfunction, asking your provider to specifically evaluate the clitoral hood is an important step. In some cases, additional assessment for underlying skin conditions like lichen sclerosus or hormonal testing may also be recommended.
Treatment Options for Clitoral Adhesions
The good news is that clitoral adhesions are treatable, and most women experience significant improvement with the right personalized care. Treatment is tailored to the severity of the adhesion, the underlying cause, and the individual's symptoms and goals.
Non-Surgical Lysis (Manual Separation)
For mild to moderate adhesions, a healthcare provider can gently separate the clitoral hood from the glans in the office. A topical anesthetic is applied first to minimize discomfort, and a fine instrument is then used to carefully break apart the fused tissue and clear away any trapped smegma or keratin pearls. This minimally invasive procedure can provide rapid relief when performed by a skilled provider. Afterward, patients are typically guided to gently retract the hood daily and maintain regular vulvar hygiene to prevent re-adhesion.
Topical Therapies
Topical estrogen is often recommended when hormonal changes have contributed to tissue thinning. Applied directly to the vulvar area, it restores tissue health, improves elasticity, and reduces the risk of recurrence. For adhesions associated with lichen sclerosus or lichen planus, topical corticosteroids help control underlying inflammation and prevent further scarring. Vulvar moisturizers and emollients used regularly support tissue hydration, reduce friction, and help maintain the tissue health needed to keep adhesions from returning.
Surgical Adhesiolysis
For severe or recurrent adhesions that do not respond to conservative management, surgical lysis under anesthesia may be recommended. This allows precise release of extensive fused tissue and is usually followed by a post-operative care plan to minimize recurrence.
The Role of Pelvic Floor Physiotherapy in Treating Clitoral Adhesions

This is where our expertise at Ova comes in and where pelvic floor physiotherapy offers something that medical treatment alone cannot provide.
Treating the adhesion itself addresses only part of the picture. Chronic clitoral pain whether from the adhesion, from the procedure used to treat it, or from years of protective tension creates lasting changes in the pelvic floor muscles, connective tissues, and nervous system. These changes must also be addressed for recovery to be complete and lasting. Our pelvic pain physiotherapy service is specifically designed for this.
Clitoral Prepuce Myofascial Release (MFR)
A specialized, evidence-informed hands-on technique where a trained pelvic floor physiotherapist applies gentle, sustained pressure and targeted stretching to the clitoral hood and surrounding connective tissue. This releases adhesions, restores natural tissue mobility, and improves the hood's ability to move freely without surgery. It is performed with full attention to your comfort, pace, and consent at every step.
Pelvic Floor Muscle Assessment and Manual Therapy
Your physiotherapist will assess the tone, coordination, and sensitivity of the pelvic floor muscles to identify any overactivity or guarding that has developed in response to chronic pain. Treatment uses gentle internal and external manual therapy, myofascial release, and muscle retraining to restore healthy function throughout the pelvis.
Nervous System Regulation
Chronic pain sensitizes the nervous system the brain learns to amplify pain signals even after the original source has been treated. Physiotherapy includes targeted strategies to calm the nervous system, gradually reduce pain sensitivity, and help the body feel safe again. This is essential for lasting improvement in sensation and sexual function.
Biofeedback
Using our biofeedback technology, you can see in real time how your pelvic floor muscles are activating and relaxing particularly powerful when muscles are tensing involuntarily in response to pain or anticipation of pain, which is very common in women with clitoral adhesions.
Breathing and Relaxation Training
The diaphragm and pelvic floor are deeply connected. Learning correct breathing patterns reduces pelvic muscle guarding, supports nervous system regulation, and helps the body release the chronic tension that amplifies pain over time.
Post-Procedure Rehabilitation
For women who have undergone lysis or surgical treatment, pelvic floor physiotherapy plays a vital role in recovery managing scar tissue mobility, supporting tissue healing, retraining muscles that have been guarded for a long time, and reducing the risk of recurrence.
Education and Self-Care Guidance
Understanding your condition changes your relationship with it. We provide guidance on safe vulvar hygiene, appropriate lubricants and emollients, daily self-care routines to maintain tissue mobility, and practical strategies to manage difficult days with confidence.
A multidisciplinary approach that combines medical care with pelvic floor physiotherapy and, where appropriate, support from a sex therapist or counsellor produces the best and most lasting outcomes.
When Should You Seek Help?
You do not need to wait until symptoms become severe. Consider reaching out for an assessment if you experience:
Clitoral pain, burning, aching, or soreness at rest or with touch
Difficulty or inability to reach orgasm, or orgasms that feel muted or different than before
Reduced clitoral sensation that has changed over time
Hypersensitivity where even light touch is uncomfortable
Pain during or after sexual activity
Visible changes to the clitoral hood or difficulty retracting it
Vulvar itching, irritation, or chronic unexplained discomfort
Symptoms that have been dismissed or left unexplained by previous providers
You deserve answers, and relief is possible.
Clitoral Adhesions Are Not a Life Sentence
Many women feel embarrassed, confused, or dismissed when they try to seek help for clitoral pain or sexual dysfunction. We want to be clear: clitoral adhesions are a recognized medical condition with real physical causes. Your symptoms are not in your head, and in most cases, they respond very well to the right treatment approach.
With a proper assessment and a personalized care plan, most women experience meaningful improvement in comfort, sensation, and intimacy. Healing is possible, and you deserve support every step of the way.
❓ FAQs About Clitoral Adhesions
-
A clitoral adhesion occurs when the clitoral hood (prepuce) fuses to the glans clitoris the sensitive tip of the clitoris preventing the hood from retracting naturally. This can trap smegma and keratin pearls underneath, causing irritation, pain, and restricted sensation.
-
More common than most people realize. Research shows they appear in approximately 22% of women presenting with sexual dysfunction and in 33% of female college students during routine exams. They are significantly underdiagnosed because clitoral examinations are not yet standard practice in most clinical settings.
-
Pain varies widely from person to person. It may present as a persistent burning, aching, or sharp sensation in the clitoral area, either at rest or triggered by touch or stimulation. Some women experience hypersensitivity; others notice numbness or a dulling of sensation. Many also notice difficulty reaching orgasm or a change in orgasmic intensity.
-
Yes. The clitoris is the primary structure involved in female orgasm, and adhesions that restrict its mobility and accessibility can significantly affect arousal and orgasmic function. Many women treated for clitoral adhesions report meaningful improvement in sensation and orgasmic capacity after treatment.
-
Treatment depends on severity and underlying cause. Options include non-surgical manual separation (lysis) by a healthcare provider, topical estrogen or corticosteroid creams, vulvar emollients, and surgical adhesiolysis for severe cases. Pelvic floor physiotherapy, including clitoral prepuce myofascial release, plays a vital role in addressing the muscular and nervous system components and supporting both recovery and prevention of recurrence.
-
Clitoral prepuce myofascial release (MFR) is a specialized hands-on technique performed by a trained pelvic floor physiotherapist. Gentle, sustained pressure and targeted stretching are applied to the clitoral hood and surrounding connective tissue to release adhesions, restore mobility, and improve tissue function without the need for surgery in many cases.
-
Absolutely. Pelvic floor physiotherapy addresses the full picture of clitoral adhesion recovery, including the pelvic floor muscle guarding, nervous system sensitization, and connective tissue changes that develop alongside chronic clitoral pain. This is essential for lasting recovery, especially when pain has been present for a long time.
-
Yes, frequently. Clitoral adhesions are commonly found alongside vulvodynia, provoked vestibulodynia, pudendal neuralgia, interstitial cystitis, and overactive pelvic floor dysfunction. This is why a thorough pelvic floor assessment is so important. Treating only the adhesion without addressing the surrounding muscle and nerve changes often leads to incomplete recovery.
-
Recurrence is possible, particularly if underlying causes such as lichen sclerosus or hormonal changes are not managed on an ongoing basis. After treatment, most providers recommend daily gentle retraction of the hood, regular use of a vulvar emollient, and appropriate topical therapy to maintain tissue health. Pelvic floor physiotherapy also supports long-term prevention by improving tissue mobility and self-care knowledge.
-
Anytime you are experiencing clitoral pain, changes in sensation, or sexual dysfunction, whether or not you have already received a medical diagnosis or procedure. Physiotherapy addresses the muscular and nervous system components that medical treatment alone cannot resolve, and supports faster and more complete recovery.
Why Choose Ova in Burnaby for Clitoral Adhesions
At Ova, we are internationally trained specialists in complex pelvic pain and women's sexual health conditions. With over 2,000 successfully treated pelvic pain cases, we bring a depth of expertise in vulvar and clitoral conditions that is rare in pelvic health care.




What Sets Ova Apart?
✅ Deep expertise in clitoral and vulvar pain
We understand the anatomy, the patterns, the co-occurring conditions, and the physical and emotional toll that clitoral adhesions take, and we treat the whole picture, not just the adhesion in isolation.
✅ Whole-person, trauma-informed care
You will be heard, believed, and treated with compassion and respect. There is no dismissal here.
✅ Evidence-informed treatment rooted in global best practices
Your care plan is built on the latest research in pelvic pain, sexual medicine, and myofascial therapy, customized to your unique presentation and goals.
✅ Specialized techniques for complex pain
Manual therapy, biofeedback, internal pelvic floor treatment, clitoral prepuce myofascial release, nervous system regulation, breathing retraining, scar tissue mobilization, and post-procedure rehabilitation all under one roof.
✅ Education that empowers you
We believe women deserve clear, honest information about their own bodies. We help you understand your symptoms, identify your triggers, and take confident control of your recovery.
Ready to Begin?
Don’t wait. The sooner we start, the sooner you can feel stronger and more supported. Space is limited due to high demand, but if you’re ready to take the first step toward lasting pelvic health, we’re here to help.
📌External References and Resources
🌐 International Society for Sexual Medicine (ISSM) – What Are Clitoral Adhesions?